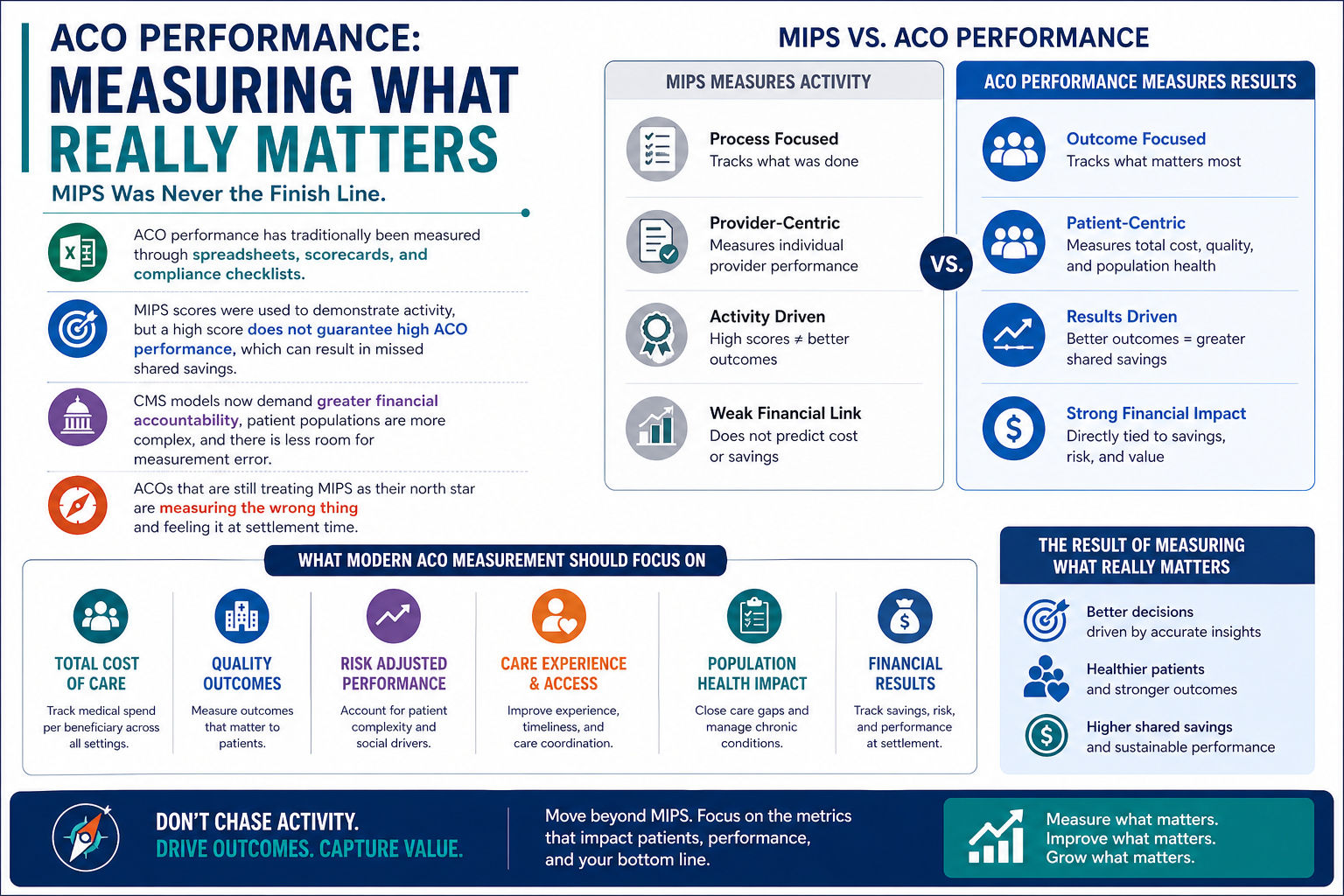
ACO performance has traditionally been measured through spreadsheets, scorecards, and compliance checklists. MIPS scores were used to demonstrate activity, but a high score does not guarantee high ACO performance, which can result in missed shared savings.
CMS models now demand greater financial accountability, patient populations are more complex, and there is less room for measurement error. ACOs that are still treating MIPS as their north star are measuring the wrong thing and feeling it at settlement time.
The Problem With MIPS-Centered Measurement
MIPS was built to reward documentation and reporting compliance, not necessarily better patient outcomes. It evaluates individual clinicians, not entire populations, which is exactly what ACOs are responsible for managing.
Where the Disconnect Shows Up
- Documentation over outcomes: A provider can score well on MIPS while a patient gets readmitted within 30 days.
- Individual vs. population lens: MIPS scores don’t reflect how well an ACO is managing chronic disease across thousands of patients.
- Lagging data: MIPS relies on historical claims, not the real-time signals needed to act early.
An ACO can be fully compliant on MIPS reporting yet still fall short of shared savings targets.
What Outcome-Based ACO Performance Actually Measures
True ACO performance is measured by control over cost, quality, and patient experience. Key indicators that drive shared savings include:
- Reduction in preventable hospitalizations and ER visits
- Chronic disease control rates across attributed populations
- Per-member-per-month (PMPM) cost vs. CMS benchmarks
- Risk-adjusted outcomes incorporating social determinants of health
- Patient attribution stability over time
These aren’t vanity metrics. They’re the exact figures CMS uses to calculate whether an ACO earns or owes money at the end of the performance year.
Key ACO Performance Barriers Holding Teams Back
ACOs rarely fail due to poor clinical care. They fail because structural and operational barriers prevent early detection and resolution of problems. Persivia’s research identifies core ACO performance barriers split across two categories.
Structural Barriers: The Blind Spots
These create gaps in visibility that prevent early intervention:
| Barrier | Impact |
| 60–90 day claims lag | Rising costs go undetected until it’s too late |
| Misaligned risk scores | Wrong patients get flagged, right ones get missed |
| Unstable attribution | Population data becomes unreliable for planning |
| Undetected high-cost patterns | Intervention windows close before action is taken |
Operational Barriers: The Slowdowns
Even when problems are identified, these barriers prevent timely action:
- Fragmented workflows spread across 10+ disconnected tools
- Manual forecasting that consistently misses CMS actuals by millions
- Delayed reporting that closes action windows before care teams respond
- No unified visibility across care coordinators, physicians, and administrators
Barriers compound each other. Claims lag combined with fragmented tools not only slows ACOs but also hinders proactive care management.
ACO Performance in 2026: What’s Actually Changing
ACO performance in 2026 is not just about better reporting. It’s about faster, smarter action on real data. The ACOs pulling ahead share a clear pattern:
- Replaced retrospective claims review with real-time risk monitoring
- Use AI-driven stratification to identify rising-risk patients weeks earlier
- Track CMS benchmark alignment continuously, not just at reporting time
- Operate from a single unified platform instead of siloed point solutions
A digital health platform connects insights to care team workflows, ensuring the right person takes timely action.
Bottom Line
ACO performance will never be fully captured by a compliance score. MIPS served a purpose, but outcome-based measurement is now the standard that separates ACOs that earn shared savings from those that don’t. The ACO Performance barriers are real, well-documented, and actively destroying shared savings potential, but they’re also solvable with the right infrastructure in place.
Persivia provides a unified AI-powered population health platform that addresses these barriers. With real-time risk stratification, reduced claims lag, stable attribution tracking, and continuous CMS benchmark monitoring, ACO teams gain the tools and visibility needed for consistent shared savings.